
WHT Report: Why It’s Difficult To Build a Good Cardiotocography Interpretation Tool Without Consensus
The Problem Is Not the Monitor. The Problem Is the way we are taught the Interpretation.


There is a persistent myth in obstetrics: that electronic fetal monitoring is a failed technology.
That cardiotocography (CTG) [aka “fetal monitoring”] has increased the cesarean rate without reducing cerebral palsy.
That it was, as some have called it, the worst test ever introduced into clinical practice.
This is wrong.
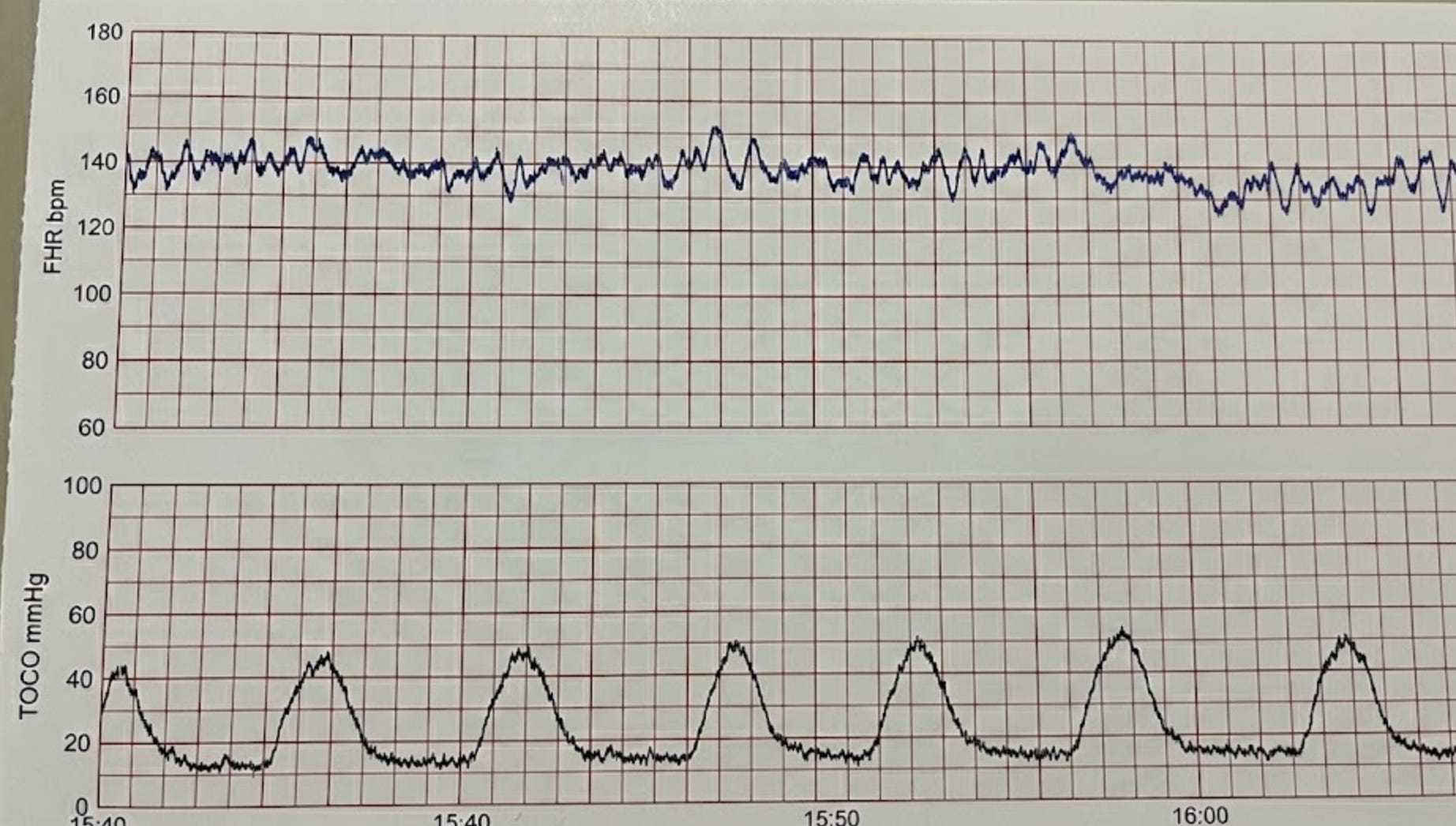
The technology is not the failure. The monitor records two channels: the fetal heart rate and uterine contractions. It does this reliably. The failure is in how we teach clinicians to interpret what the monitor shows, and specifically, how we are being taught interpretation.
A new paper in Obstetrics & Gynecology makes this painfully clear. The authors compared ACOG (The American College of Obstetricians and Gynecologists) and AWHONN (The Association of Women's Health, Obstetric and Neonatal Nurses) guidelines across fetal heart rate interpretation, uterine activity, oxytocin management, and labor management. They found 14 areas of disagreement against 8 of agreement. But the real story is not the count.
It is what the disagreements reveal about whose interests each organization serves.
The Monitor Is Not the Problem. The Interpretation Is.
Cardiotocography records two signals that must be read together. A fetal heart rate deceleration means one thing in the context of normal contractions and something entirely different during tachysystole. The contraction channel is not decoration. It is half the diagnostic information.
Here is where we have failed. ACOG’s interpretation framework, the three-tier category system, focuses almost entirely on the fetal heart rate. Uterine activity gets a passing mention. ACOG does not define what constitutes excessive contraction duration, elevated resting tone, or inadequate relaxation time between contractions. The only uterine activity parameter ACOG recognizes is the NICHD definition of tachysystole: more than five contractions in 10 minutes.
That is like reading an EKG and ignoring the rhythm strip.
AWHONN, by contrast, defines specific uterine activity parameters that clinicians can measure and act on: contractions lasting two minutes or longer, resting tone above 25 mmHg by IUPC, relaxation time under 60 seconds in the first stage and under 45 seconds in the second stage. These are concrete, measurable criteria. You can teach them. You can program them. You can build a clinical decision support tool around them.
ACOG’s silence on uterine activity parameters is not restraint. It is an interpretation framework with a blind spot in one eye.
The Women's Health Tech Report: Safety analysis, the evidence critique, and the verdict are below -- for subscribers who want the full picture. The following includes an interactive tool to help you understand the differences among interpretations.
