
When Ovulation Stops: Understanding Amenorrhea as the Body’s Survival Reflex
The Obstetric Intellect - Menstruation follows ovulation, not the other way around. When ovulation ceases—whether in pregnancy, starvation, or stress—the body is protecting life, not failing it

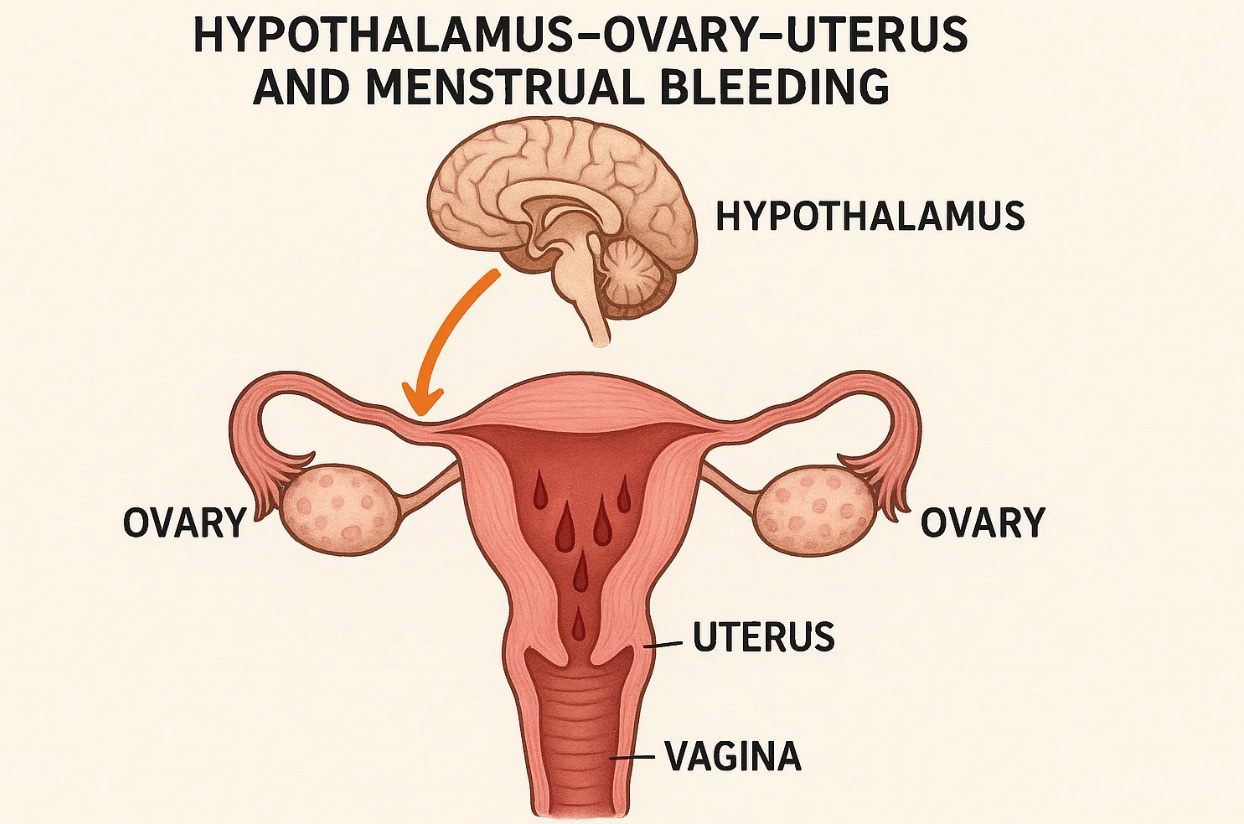
Menstruation follows ovulation, not the other way around. Every menstrual cycle begins not in the uterus but first in the brain, then the ovary and finally the uterus. When the brain tells the ovary not to ovulate, not to release the egg, when ovulation stops or occurs less often, menstruation stops too. The regular monthly bleeding that most women call a “period” or “menstruation” is the body’s signal that ovulation has occurred, fertilization did not, and the uterine lining is being shed. Women can bleed and spot without ovulation, but when it’s not regular, it’s not regular menstruation, it’s not a “period”.
Period (Menstrual Period): A period is the monthly bleeding that follows ovulation when pregnancy has not occurred. It results from the shedding of the uterine lining as hormone levels fall. True menstruation requires prior ovulation; bleeding without ovulation is not a true period but anovulatory bleeding.
Ovulation is the release of an egg from the ovary, triggered by a mid-cycle surge in luteinizing hormone (LH). It marks the moment when reproduction is possible.
Menorrhea or Menstruation, by contrast, is the shedding of the endometrial lining approximately two weeks later if pregnancy has not occurred. Without ovulation, there is no luteal phase, no progesterone withdrawal, and therefore no true menstrual bleeding.
This sequence explains why pregnancy and menopause themselves are a physiologic (“normal”) form of amenorrhea, of missing a regular period. Once conception occurs, ovulation halts—human chorionic gonadotropin (hCG) and high progesterone levels suppress the hypothalamic-pituitary-ovarian axis to maintain the uterine lining and prevent further ovulation. In a normal pregnancy, menstruation ceases because the hormonal cycle that drives it is intentionally interrupted. Any bleeding that occurs during pregnancy is not menstruation but abnormal uterine bleeding from implantation, placenta, or cervical changes.
Here are medical terms for abnormal menses/periods
Amenorrhea: Absence of menstrual periods—can be primary (never started) or secondary (stopped after previously normal cycles).
Hypomenorrhea: Unusually light or scant menstrual bleeding.
Oligomenorrhea: Infrequent menstrual periods, typically occurring more than 35 days apart.
Polymenorrhea: Abnormally frequent menstrual cycles, usually less than 21 days apart.
Menorrhagia: Excessive or prolonged menstrual bleeding at regular intervals.
Metrorrhagia: Bleeding between periods or at irregular intervals.
Menometrorrhagia: Heavy and irregular bleeding, combining features of menorrhagia and metrorrhagia.
Dysmenorrhea: Painful menstruation, often associated with cramping or pelvic discomfort.
The Physiologic Sequence: From Brain to Bleeding
In a healthy, ovulatory cycling woman, the hypothalamus releases GnRH in rhythmic pulses. The pituitary responds by secreting FSH and LH, which stimulate the ovaries to mature follicles and produce estrogen. Around mid-cycle, the LH surge triggers ovulation—the release of an egg. Afterward, the follicle becomes the corpus luteum, secreting progesterone that stabilizes the uterine lining in anticipation of pregnancy.
If fertilization does not occur, progesterone levels fall. The endometrium loses its hormonal support and breaks down, resulting in menstrual bleeding—the visible endpoint of a cycle that began weeks earlier in the brain.
When energy deficiency, psychological stress, or disease disrupts this sequence, the hypothalamus stops releasing GnRH. Without that pulse, the pituitary does not release LH or FSH, and the ovary does not ovulate. Without ovulation, the uterine lining remains thin, and menstruation ceases. The result is amenorrhea, a visible sign of invisible anovulation.
The Body’s Emergency Mode
My mother, imprisoned by the Nazis during World War II, stopped menstruating within months of arrival in the camps. She believed, as many did, that the Nazis had injected women with hormones to prevent fertility. In truth, no injection was necessary. Her ovulation had stopped because her body, starved and terrified, had no resources to sustain reproduction. Also, when she lost weight, ovulation stopped. What she experienced was functional hypothalamic amenorrhea—the brain’s emergency command to halt ovulation and conserve energy.
Studies of Holocaust survivors later confirmed this pattern. Nearly all menstruating women stopped ovulating and bleeding shortly after internment, a direct consequence of starvation and extreme stress. Menstrual cycles typically resumed months after liberation when nutrition and safety and normal weights returned. For many, the first period after the war was a deeply emotional event—a physiological declaration that life had resumed. And consequently there was an increase in fertility.
Primary ovarian insufficiency (POI), Perimenopause, and Menopause
Primary ovarian insufficiency (POI) previously known as Premature ovarian failure—occurs when the ovaries stop functioning before age 40, leading to irregular or absent ovulation and amenorrhea due to depleted or unresponsive follicles.
In contrast, perimenopause is the natural transitional phase leading up to menopause, characterized by fluctuating hormone levels, irregular ovulation, and variable bleeding patterns such as oligomenorrhea or menometrorrhagia.
Menopause is defined retrospectively after 12 consecutive months without menstruation, reflecting the permanent cessation of ovulation and estrogen production. These stages represent a continuum of declining ovarian activity and mark the gradual end of reproductive capacity.
The Modern Mirror: Athletes and Amenorrhea
The same biology operates today under different names. In athletes, dancers, and women with eating disorders, ovulation often stops when energy intake cannot meet physical demands. This athletic amenorrhea arises from the same hypothalamic suppression seen in famine. Low energy availability signals the brain that it cannot afford reproduction. Ovulation ceases, estrogen falls, and menstruation disappears.
This is not a benign adaptation. Estrogen deficiency leads to loss of bone mineral density, stress fractures, and premature osteoporosis. The so-called female athlete triad—low energy availability, amenorrhea, and low bone mass—remains a major health risk. In adolescents, it can permanently impair peak bone formation. Fertility usually returns when ovulation resumes, but chronic suppression may leave lasting skeletal and endocrine effects.
Over time, prolonged hypothalamic suppression can mimic or mask premature ovarian insufficiency (POI), a condition in which the ovaries themselves fail to produce normal levels of estrogen and viable follicles before age 40. In true POI, ovarian reserve is depleted or the follicles no longer respond to gonadotropins, leading to persistently elevated FSH and irreversible amenorrhea. In contrast, athletic or stress-related amenorrhea reflects a reversible central (hypothalamic) suppression of otherwise normal ovaries.
While most athletes with functional hypothalamic amenorrhea do not have true POI, years of undernutrition and hormonal suppression may accelerate follicular loss or unmask underlying ovarian vulnerability. If menses and ovulation do not resume after nutritional rehabilitation and normalization of weight, evaluation for POI becomes essential. In these cases, the distinction is both diagnostic and prognostic: hypothalamic amenorrhea can recover, but POI signifies permanent loss of ovarian function and early estrogen deficiency with implications for bone, cardiovascular, and cognitive health.
Thus, the absence of menstruation in athletes should never be dismissed as a normal effect of training. Whether temporary or permanent, it signals a disturbance in the reproductive axis that demands investigation and, when possible, restoration of ovulatory function.
Pregnancy, Ovulation, and the Meaning of Normal
Pregnancy itself is the best illustration of the link between ovulation and menstruation. During pregnancy, the ovary’s corpus luteum and then the placenta produce high levels of estrogen and progesterone, maintaining the uterine lining and suppressing new ovulation. The absence of menses in pregnancy is entirely normal because the reproductive system has already succeeded in its goal—life is growing, and another ovulation is unnecessary.
Outside pregnancy, however, the absence of menstruation almost always means one thing: no ovulation. The causes may vary—starvation, stress, endocrine disease, or athletic overexertion—but the physiology is identical.
In each case, the absence of bleeding is not just a gynecologic event but a systemic one. The body is making a trade-off: conserving calories, diverting energy to vital organs, and deferring reproduction until conditions improve.
Amenorrhea Is a Message
Amenorrhea, whether from pregnancy, trauma, or overtraining, is the body’s way of communicating priorities. It says: Not now. Not until it’s safe. The mechanism is ancient and protective, but modern culture often misreads it. When a woman misses her period and is not pregnant, the absence is not “normal.” It is a sign that the body’s hormonal axis has withdrawn reproductive permission.
In clinical practice, distinguishing true menstruation from other bleeding is crucial. Menstrual bleeding follows ovulation and hormonal withdrawal; anovulatory bleeding may occur unpredictably from endometrial instability without prior ovulation. This distinction is central to diagnosis and management. A woman can bleed without ovulating, but she cannot menstruate without ovulating first.
Ethics and the Language of Health
For my mother, amenorrhea in Auschwitz symbolized deprivation and survival. For athletes and patients today, it often reflects social and cultural pressures to overperform and undernourish. In both settings, the physiology is the same—only the context differs.
Physicians must teach this clearly: menstruation is not a nuisance, and its absence is never trivial. Whether due to pregnancy, stress, or starvation, amenorrhea reveals the body’s priorities. Our role is to interpret that signal, not ignore it.
Reflection
When ovulation stops, the body is protecting itself. Menstruation disappears not because something “went wrong,” but because the reproductive system is wise enough to wait. Pregnancy proves this principle beautifully—when life is already being created, ovulation stops naturally. But when life feels threatened, ovulation stops for the same reason: to safeguard what remains.
In both cases, the absence of bleeding is an act of preservation. The return of ovulation, whether after pregnancy, famine, or recovery, marks the body’s declaration that safety has been restored.
Menstruation follows ovulation. Understanding that sequence transforms how we view both fertility and health. The uterus does not decide when to bleed; the brain decides when it is safe to create life.