
INTRODUCTION TO "THE WOMEN’S HEALTH TECH REPORT"
By Amos Grunebaum, MD | ObGyn Intelligence | obmd.com


Introductory Issue — Free to All Readers
Why I'm Writing This
For a year, ObGyn Intelligence has been cutting through the noise in women's health. Now it's time to do the same for the technology that is changing it.
About a year ago, I started ObGyn Intelligence -- a newsletter built on a simple premise: evidence matters in women's health, and there is far too much noise drowning it out. Since then, the response has been more than I expected. Clinicians, researchers, patients, and educators have found it and kept coming back. The newsletter has grown into something I am genuinely proud of, and the conversations it has started -- in comments, in emails, in clinical hallways -- have confirmed what I suspected when I launched it: there is a real hunger for honest, evidence-based analysis of women's health that does not talk down to its readers and does not pull its punches.
Over the past several months, many of you have asked the same question in different forms.
What do I think about AI in obstetrics and in gynecology. In Women’s Health?
What about the fertility apps patients keep bringing up in appointments?
What about the fetal monitoring algorithms, the maternal early warning systems, the chatbots patients are using to interpret their own lab results?
What about patient safety issues?
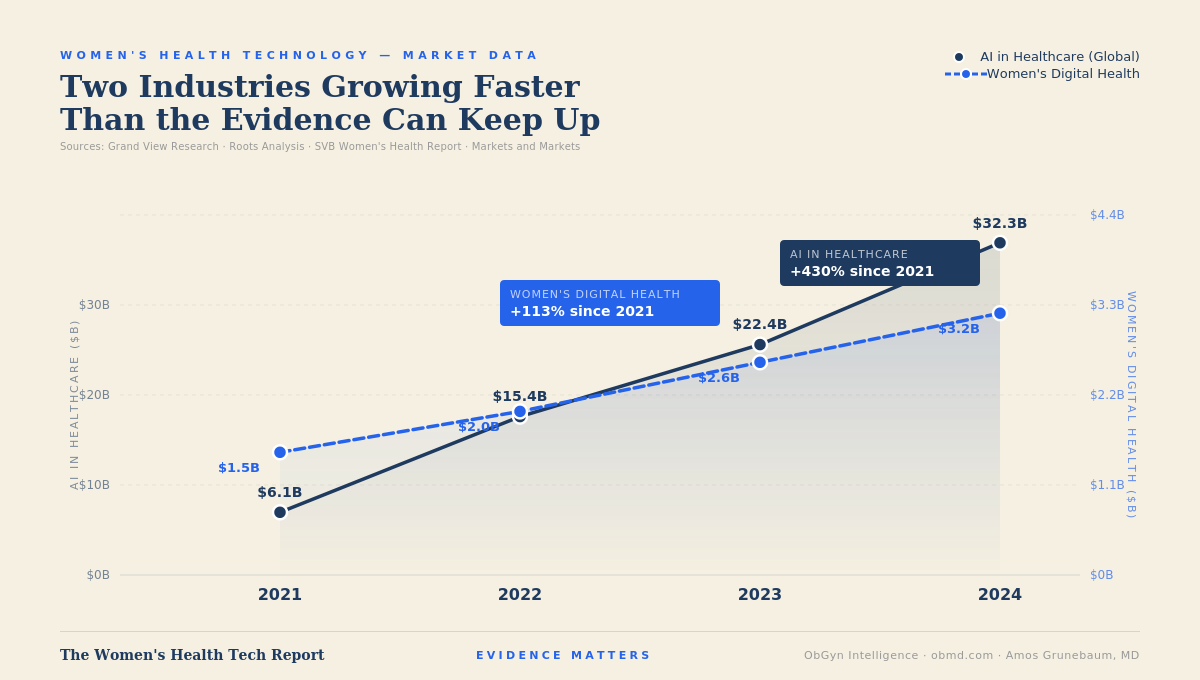
Is this technology actually helping, or is it moving faster than the evidence can keep up with?
Those are exactly the right questions. And they deserve their own dedicated space.
This is that space.
What The Women's Health Tech Report Is
The Women's Health Tech Report publishes two to three times per week as a dedicated series within ObGyn Intelligence. Each issue covers technology in depth -- one honest assessment of what the evidence actually shows, what the tool actually does, and where it fails. No press releases. No vendor language. No cheerleading for technology that has not earned it.
The technologies covered here span the full landscape: artificial intelligence, clinical algorithms, diagnostic software, consumer health apps, wearable devices, fertility technology, and anything else that touches women's health in the clinic or at home. Some of it is genuinely transformative. Some of it is harmful. Most of it sits somewhere in between, deployed with confidence that the evidence does not yet support.
That gap is the reason this series exists.
Why This Matters Now
Health technology is entering women's care at a pace the regulatory and clinical evaluation systems were not built to handle. The FDA clears AI-enabled medical devices through pathways designed for traditional hardware. Peer review of clinical algorithms is inconsistent and often proprietary. Consumer health apps operate almost entirely outside any clinical evidence standard. And patients are encountering all of it -- in their clinics, on their phones, in their hospital rooms -- without anyone explaining what it does and does not do.
The result is a landscape where a hospital can deploy a maternal early warning algorithm without a published bias audit. Where a patient can receive an AI-generated fetal risk score without knowing how that score was calculated or validated. Where a fertility app can claim clinical accuracy without a single peer-reviewed study.
This is not theoretical. These things are happening now, in clinical settings, to real patients. The consequences range from missed diagnoses to unnecessary interventions to the perpetuation of existing disparities in care. Women deserve better than that.
Who I Am and Why I'm the Right Person to Write This
I have practiced obstetrics and maternal-fetal medicine for more than 50 years. I have watched technology enter clinical medicine in waves -- the introduction of electronic fetal monitoring, the ultrasound revolution, the genomics era, and now the AI moment.
Each wave brought genuine advances and genuine harms, often arriving together and often indistinguishable from each other until the evidence caught up.
I am an active researcher using the CDC natality database, one of the most comprehensive sources of population-level birth outcome data available. I am a peer reviewer for major obstetric journals. I co-developed the preventive ethics framework for obstetric practice. I have spent decades studying the gap between what clinical trials show and what actually happens to patients at scale.
I am not neutral about bad evidence. I am not impressed by a well-designed press release. I am not persuaded by the argument that a technology must be good because it is new. And I have seen enough catastrophic outcomes in obstetric care to know that a tool that performs well in a controlled validation study can fail the patient in room 4 in ways the study never measured and the developer never anticipated.
—→ My job in this series is to tell you what the technology actually does -- not what its developers say it does, not what the hospital administrator who approved the purchase believes it does, not what the algorithm says about itself.
Who This Is For
For ObGyns and other Clinicians
This series is for clinicians who want to evaluate health technology with the same rigor they apply to drug trials. A new medication requires demonstrated efficacy, safety data, dose-response characterization, and post-market surveillance. A clinical algorithm that drives the same decisions should meet the same standard. Most do not. This series will tell you which ones fall short and what to look for.
For Patients and anyone else interested in Tech
It is for patients who are encountering AI-generated health information, fertility apps, wearable monitors, and chatbot medical advice and deserve an honest assessment of what to trust and what to question. The information asymmetry between what technology developers know about their products and what patients know is not acceptable when the stakes are maternal and fetal health.
It is for anyone who believes that evidence matters in women's health -- because in this space, the gap between what technology promises and what it delivers is not a minor inconvenience. It is a patient safety issue.
What Free Readers Get, What Paid Subscribers Get
Every issue covers one technology. Free readers receive the technology description and the clinical context -- what the tool is, what it is supposed to do, and how it is being used. Paid subscribers receive the safety analysis, the evidence critique, and the bottom line. That is where the work is, and it is what the subscription supports.
If you are already a paying subscriber to ObGyn Intelligence, you are already in. This series is included.
What Comes Next
The first issues focus on artificial intelligence because AI is the dominant story in health technology right now and because the stakes are highest where adoption is fastest. Issue 1 examines AI interpretation of fetal heart rate tracings in labor. Issue 2 examines a documented algorithmic failure in maternal risk prediction. Issue 3 examines how patients are using AI chatbots in pregnancy and what clinicians need to know about it.
From there the series expands to cover the full landscape: consumer fertility technology, wearable monitoring devices, genetic testing platforms, clinical decision support tools, digital therapeutics, and whatever else arrives that is being deployed in women's health faster than the evidence can evaluate it.
If you are a clinician using a technology in your practice that deserves scrutiny, write to me. If you are a patient who has encountered a health technology that raised questions about accuracy, safety, or transparency, write to me. The most important evidence in this field often starts in the clinic, not the journal.
I am glad you are here.
Amos Grunebaum, MD
The Women's Health Tech Report | ObGyn Intelligence | obmd.com
Why I am here
Women’s health technology is moving fast. Too fast for most clinicians to evaluate, and too fast for most patients to navigate alone. This report publishes two to three times per week -- not to celebrate every new tool, but to ask the question nobody else in this space is asking: does the evidence actually support what this technology claims to do?
If something in this issue changed how you think about a tool, a system, or a conversation with a patient -- forward it to one colleague who needs to read it. That is how this reaches the people it is meant for.
Already a subscriber? Thank you. If someone sent this to you, you can subscribe free at obmd.com.