
"Social Determinants of Health" Functions as a Smokescreen. Here Is What It Obscures.
Eleven papers document associations between neighborhood deprivation and adverse outcomes. Not one makes insurance differences ts primary exposure. Not one acknowledges the elephant in the room.

Eleven papers from Obstetrics & Gynecology document associations between neighborhood deprivation and adverse outcomes. Not one makes Medicaid versus private insurance its primary exposure. That is a choice, not a gap.
The February 2026 Issue of Obstetrics & Gynecology
The February 2026 issue of Obstetrics & Gynecology is instructive. Kawakita and colleagues published a rigorous cohort study of 61,008 pregnancies, finding that patients in the most deprived neighborhoods by the Area Deprivation Index faced a threefold increased risk of stillbirth compared to patients in the least deprived quartile (RR 3.08, 95% CI 1.74-5.44). (1) The accompanying editorial by Silver covered eight pages on the subject. (2) Neither piece uses the word ‘Medicaid’ as a substantive variable. Neither asks what share of the high-ADI cohort was publicly insured, what obstetric care looks like under Medicaid reimbursement in Virginia, or whether the risk gradient would persist if reimbursement parity were achieved.
This is not a criticism of either paper in isolation. It is a pattern. Across eleven recent papers in Obstetrics & Gynecology and its supplements, the phrase ‘social determinants of health’ appears hundreds of times. The phrase ‘Medicaid reimbursement’ appears zero times. ‘Public insurance’ appears as a demographic covariate, listed alongside age, race, and parity, not as an exposure whose specific attributes might explain what we are seeing.
A language choice this consistent is not accidental. It reflects how the field has decided to frame a problem that has a more specific answer than the framing suggests.
What the Eleven Papers Show
The papers reviewed here cover stillbirth, LARC removal, postpartum visit attendance, BV reinfection, hysterectomy outcomes, doula care, SDOH screening, neighborhood deprivation and birth weight, language discordance, and ACOG’s committee statement on structural determinants of health. (1-11) Together they document genuine associations between socioeconomic disadvantage and worse obstetric outcomes. The evidence is solid. The ADI predicts stillbirth. Transportation barriers predict LARC removal difficulty. Neighborhood deprivation predicts preterm birth and low birth weight. Food insecurity is near-universal in high-risk obstetric populations.
What none of these papers does is ask the next question: why do people in deprived neighborhoods receive structurally different obstetric care from people in non-deprived neighborhoods?
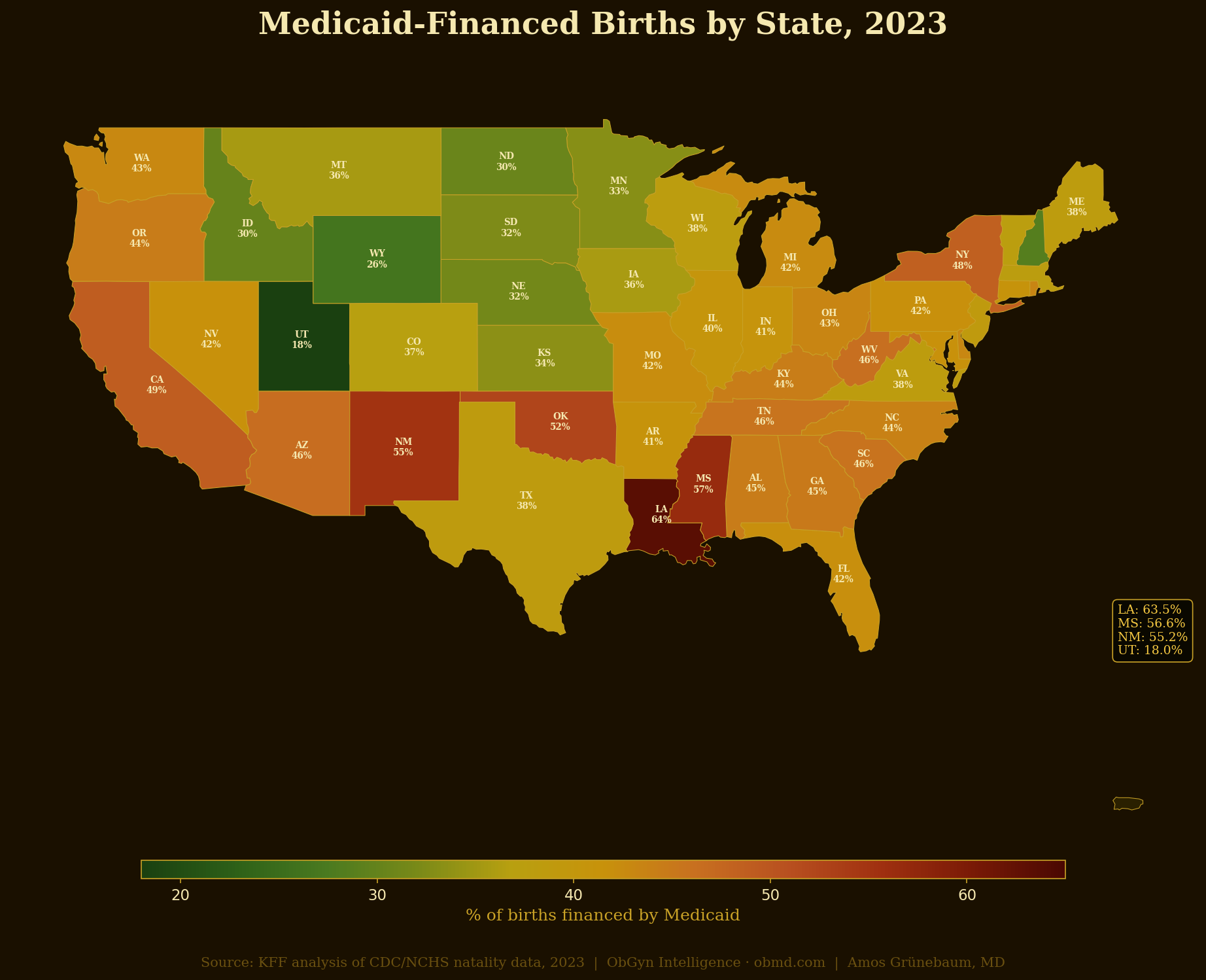
The answer is not difficult to find if you ask it. The most reliable sorting mechanism for obstetric care quality in the United States is insurance type. Medicaid covers approximately 42% of all U.S. births. [VERIFY: current Medicaid birth share] Medicaid reimburses obstetricians at rates 30 to 50% below Medicare and 60 to 70% below private insurance in most states. The result is predictable and well-documented: below 50% of obstetricians in many states accept Medicaid. Patients in high-ADI neighborhoods are disproportionately Medicaid-insured. The correlation is not incidental.
The ACOG Committee Statement No. 11 on Addressing Social and Structural Determinants of Health in the Delivery of Reproductive Health Care is the most comprehensive framing document reviewed here. (5) It is eight pages long. It contains 38 references. The word ‘Medicaid’ does not appear. The word ‘insurance’ appears twice, in the context of screening tools and not as a structural variable. The Statement recommends screening for social needs, establishing medical-legal partnerships, accommodating transportation barriers, and advocating for policy change. These are reasonable recommendations. They do not name the mechanism that creates most of the disparity they are addressing.
The Signal in the Data They Did Report
Several of the papers reviewed inadvertently illuminate the insurance gap even while not studying it directly.
Class and colleagues examined postpartum visit attendance in a high-risk inner-city sample. (3) Among 3,684 births, 70.3% used public health insurance. After adjustment, public insurance was associated with 39% lower odds of 6-week visit attendance (OR 0.61, 95% CI 0.50-0.74). This finding is presented as a covariate. The paper’s recommendations center on telemedicine and transportation support. There is no analysis of what distinguishes the care available to the 70% publicly insured from the care available to the remaining 30%.
Sato and colleagues examined bacterial vaginosis reinfection in Chicago and found that Medicaid and Medicare patients had significantly higher rates of multiple positive BV results (P<.001). (8) The conclusion focuses on access to fruits and vegetables, which showed a modest protective association. Medicaid status is listed as a finding, not explored as a mechanism.
Hall and colleagues found that patients with one or more social determinants of health had more than twice the odds of reporting difficult LARC removal, with transportation barriers showing the largest effect (aOR 2.90, 95% CI 1.07-7.87). (4) The recommendation is to consider SDH at the time of contraceptive selection. There is no analysis of whether Medicaid’s transportation benefit adequacy, which varies dramatically by state, might explain part of the transportation barrier finding.
In the Tillemann study of cesarean delivery outcomes at a large academic system, Black patients were 55% publicly insured compared to 21% of White patients (P<.05). (6) Racial disparities in labor duration, chorioamnionitis rates, and hospital stay length were documented. Insurance type was adjusted for in the demographic table but not analyzed as a potential mediator of those disparities
.Why the Exposure Variable Matters
Kahneman’s work on cognitive framing is useful here. The choice of exposure variable focuses attention and shapes what questions get asked. When researchers use the Area Deprivation Index, they focus attention on neighborhood characteristics: education levels, employment rates, housing quality, poverty concentration. These are real and important. They are also upstream of the actual care encounter.
When the exposure variable is insurance type, a different set of questions becomes visible: Which providers in this neighborhood accept Medicaid? What is the visit time allowed under the prevailing Medicaid managed care contract? Is fetal surveillance reimbursed at rates that make it economically viable to offer? Is enhanced antenatal monitoring for high-ADI patients financially sustainable for a practice that sees predominantly Medicaid patients?
The ADI tells us where the problem is concentrated. It does not tell us what created the disparity in care. Insurance type does not tell us everything either, but it is the most proximate, measurable, and policy-modifiable variable linking socioeconomic disadvantage to obstetric care quality. It also implicates specific legislators, specific reimbursement schedules, and specific contract decisions, which may be precisely why it is less studied.
Marcus Aurelius wrote that we suffer more in imagination than in reality. The inverse is true here. The suffering is real. The imagination needed is of a more precise causal model, one that is willing to name the mechanism.
What Sufficiency Requires
Evidence-based medicine requires that we distinguish between the factors we can measure and the mechanisms we propose. The papers reviewed here are methodologically sound. The ADI reliably predicts stillbirth. Transportation barriers reliably predict LARC removal difficulty. Food insecurity reliably predicts poor obstetric outcomes.
What remains underspecified is the causal chain connecting these associations to a policy target.
Sufficiency in this literature would require at least the following. First, direct comparison of outcomes by insurance type as a primary exposure, not a demographic covariate. Second, analysis of whether the ADI-outcome gradient persists after stratification by insurance type, which would tell us how much of the neighborhood effect is mediated by insurance access. Third, study of natural experiments: states that expanded Medicaid, states that increased Medicaid obstetric reimbursement, states that mandated Medicaid coverage of doula services. Fourth, honest engagement with the participation rate problem: in a high-ADI census tract, what fraction of obstetricians accept Medicaid, and what does that mean for access to the enhanced surveillance that Kawakita and Silver recommend?
The Kawakita paper itself gestures in this direction. In its discussion section, it mentions ‘enhancing Medicaid transportation benefits’ and ‘expanding perinatal mental health services’ as possible interventions. (1) These are the right levers. But they appear as recommendations appended to a study that did not examine Medicaid as an exposure, which means there is no analysis supporting the connection between the intervention and the outcome. The leap is inferential, not evidential.
The Language We Choose
‘Social determinants of health’ is not a false concept. The conditions in which people are born, live, and work genuinely shape health outcomes. The criticism is not of the concept but of its use as a terminal explanation rather than a starting point for more specific analysis.
When we say a patient’s stillbirth was associated with neighborhood deprivation, we are describing a correlation. When we ask why patients in deprived neighborhoods have worse stillbirth outcomes despite presenting to the same hospital system, we are approaching explanation. When we examine whether those patients received equivalent antenatal surveillance, equivalent fetal monitoring, equivalent timely access to specialist care, and whether the answer to any of those questions is no, and whether the reason is reimbursement-driven provider behavior, we are approaching the mechanism.
The literature reviewed here stops reliably at the correlation stage. ACOG Committee Statement No. 11 stops at the intervention stage, recommending responses to named social needs without analyzing why those needs disproportionately affect patients in the health system’s care. Neither fully engages the mechanism stage.
The word ‘Medicaid’ is not missing from these papers because Medicaid is irrelevant. It is missing because naming it would change the nature of the required response. Screening a patient for food insecurity is something an obstetrician can do in clinic. Changing Medicaid reimbursement rates requires legislative action, managed care contract reform, and sustained political will. The first response fits within existing clinical infrastructure. The second does not. That asymmetry shapes what gets studied and what gets recommended.
Autonomy is not strengthened by silence. Patients in high-ADI neighborhoods deserve to know not only that their neighborhood predicts risk but why their neighborhood predicts risk, and what specific systemic decisions created that prediction. That requires naming the mechanism. The mechanism has a name.
The Fix Is Known. The Will Is Missing.
Achieving insurance parity is tractable in a way that eliminating poverty is not. Medicaid reimbursement rates are set by legislators and updated by regulators. Provider participation follows reimbursement. A state that raises Medicaid obstetric fees to 90% of private rates can measure the effect on participation within one contract cycle. A state that mandates coverage parity for fetal surveillance, antenatal visits, and postpartum care can track whether visit rates and outcomes change.
These are policy levers with known mechanisms and measurable outcomes. "Social determinants of health," by contrast, encompasses poverty, education, housing, food security, and neighborhood infrastructure. Eliminating them requires generational investment across sectors that medicine does not control. If the goal is reducing obstetric disparity within a policy timeframe that matters to living patients, insurance type is the right target. ACOG knows this.
The Committee Statement that omits the word "Medicaid" in eight pages on structural determinants of reproductive health care was not written by people unfamiliar with reimbursement policy. The omission is not ignorance. ACOG's membership includes the practices and health systems whose revenue depends on the current reimbursement structure.
Naming Medicaid as the proximate driver of obstetric disparity would require ACOG to advocate for the reimbursement increases that would reduce that disparity, at the expense of members who have built their practices around the existing differential.
That is a conflict the Statement does not acknowledge and the literature does not examine.
Bottom Line
Eleven papers in Obstetrics & Gynecology document that neighborhood deprivation predicts adverse obstetric outcomes. The evidence is solid. The analytical framework is incomplete. The most proximate, measurable, and policy-modifiable driver of care disparities in these populations is insurance type, specifically the structural differences between Medicaid and private insurance coverage in terms of reimbursement rates, provider participation, visit time, and access to surveillance. Not one of the eleven papers analyzes insurance type as a primary exposure. ACOG Committee Statement No. 11 does not mention Medicaid in eight pages on structural determinants of reproductive health care. This is not a research gap. It is a framing choice, and framing choices have consequences for what policy solutions become visible.
References
1. Kawakita T, Hayasaka M, Harper AM, Brush J, Saade G. Association between neighborhood social determinants of health and stillbirth. Obstet Gynecol 2026;147:139-47. doi: 10.1097/AOG.0000000000006115
2. Silver RM. Social determinants of health and stillbirth: time for the next-generation. Obstet Gynecol 2026;147:137-38.
3. Class QA, Oyelola OTP. Postpartum well-visit attendance: how residential distance and social determinants of health may be associated with care [Abstract]. Obstet Gynecol 2025;145(6 Suppl):31S.
4. Hall BE, Atrio J, Evans TA, Danvers A. Social determinants of health and patient-reported difficult removal of long-acting reversible contraception [Abstract]. Obstet Gynecol 2024;143(5 Suppl):9S.
5. American College of Obstetricians and Gynecologists. Addressing social and structural determinants of health in the delivery of reproductive health care. Committee Statement No. 11. Obstet Gynecol 2024;144:e113-e120.
6. Tillemann LB, Campbell OP, Baker KA, et al. The effect of race on interventional thresholds in patients undergoing cesarean deliveries [Abstract]. Obstet Gynecol 2025;145(6 Suppl):17S.
7. Colley D, Haq K, Rodriguez AR, et al. Effect of doula care on social determinants of health: doulas as a tool to address nonmedical health care disparities within the health care system [Abstract]. Obstet Gynecol 2025;145(6 Suppl):17S.
8. Sato AJ, Tchernodrinski TS, Shi E, et al. The social determinants of health and bacterial vaginosis reinfection in Chicago, Illinois [Abstract]. Obstet Gynecol 2025;145(6 Suppl):58S.
9. Hare AM, Tappy E, Schaffer JI, et al. Effects of social determinants of health and social support on surgical outcomes among patients undergoing hysterectomy. Obstet Gynecol 2025;145:115-23. doi: 10.1097/AOG.0000000000005771
10. McCray J, Rafferty-Millett T, Shamoun R, Wilkie G. Screening for social determinants of health among pregnant patients with diabetes [Abstract]. Obstet Gynecol 2025;145(6 Suppl):14S.
11. Witsoe M, Mickelson K, Krzyzanowski B, et al. Assessing neighborhood deprivation on birth outcomes: a study of low birth weight in Phoenix, Arizona [Abstract]. Obstet Gynecol 2025;145(6 Suppl):14S.