
Precision Without Prevention: Why Language in Fetal Monitoring Matters for Patient Safety, Clinical Judgment, and Malpractice Risk
Despite decades of use, fetal monitoring remains one of the most debated and litigated areas in medicine. And is called "the worst test in medicine."

Introduction
Electronic fetal monitoring (MF) or better defined as cardiotocography (CTG) is one of the most widely used technologies in modern obstetrics.
It documents uterine contractions and the fetal heart rate.
Nearly every hospital labor unit in the United States relies on cardiotocography to monitor maternal and fetal well-being during labor.
Yet despite decades of use, fetal monitoring remains one of the most debated and litigated areas in medicine.
In response to inconsistent interpretation, obstetrics attempted to solve the problem with standardized terminology. The National Institute of Child Health and Human Development consensus system introduced clear definitions for baseline fetal heart rate, variability, accelerations, decelerations, and uterine tachysystole. These definitions were incorporated into professional guidance to replace vague expressions such as “fetal distress.”
The goal was admirable and necessary. If clinicians described tracings using the same language, communication would improve and patient safety would follow.
But an uncomfortable truth remains. Standardized terminology improved description. It did not solve the deeper challenge of recognizing early physiologic deterioration during labor.
This gap between terminology and physiology has consequences. In clinical care it may delay preventive action. In malpractice litigation it can create vulnerability for clinicians whose reasoning is not clearly documented.
Understanding this distinction is therefore not theoretical. It is an essential clinical skill.
Why standardized language became necessary
Before consensus terminology, fetal monitoring interpretation was often subjective. Clinicians used phrases such as:
fetal distress
non-reassuring tracing
intolerance of labor
These terms were widely understood but poorly defined. Different clinicians could interpret the same tracing very differently.
This lack of standardization created serious problems in labor management. Communication between nurses and physicians could break down. Residents might describe tracings differently from attending physicians. Documentation often failed to capture the clinical reasoning behind decisions.
The NICHD consensus terminology attempted to correct this by defining observable features of the tracing. These included:
baseline fetal heart rate
variability
accelerations
early, variable, and late decelerations
uterine activity
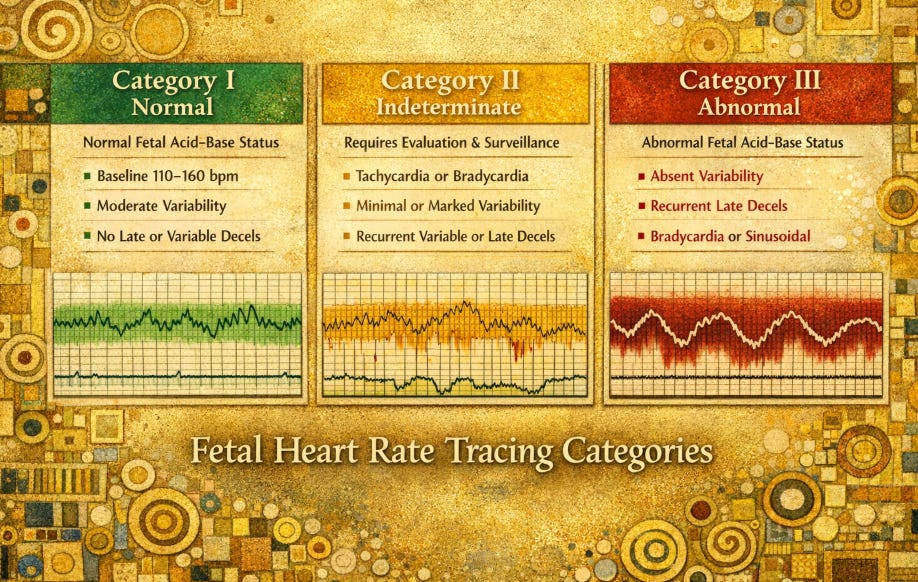
These observations were integrated into a three-tier system:
Category I patterns predictive of normal fetal acid-base status
Category II indeterminate patterns
Category III patterns associated with increased risk of fetal acidemia
ACOG / NICHD Fetal Heart Rate Tracing Categories
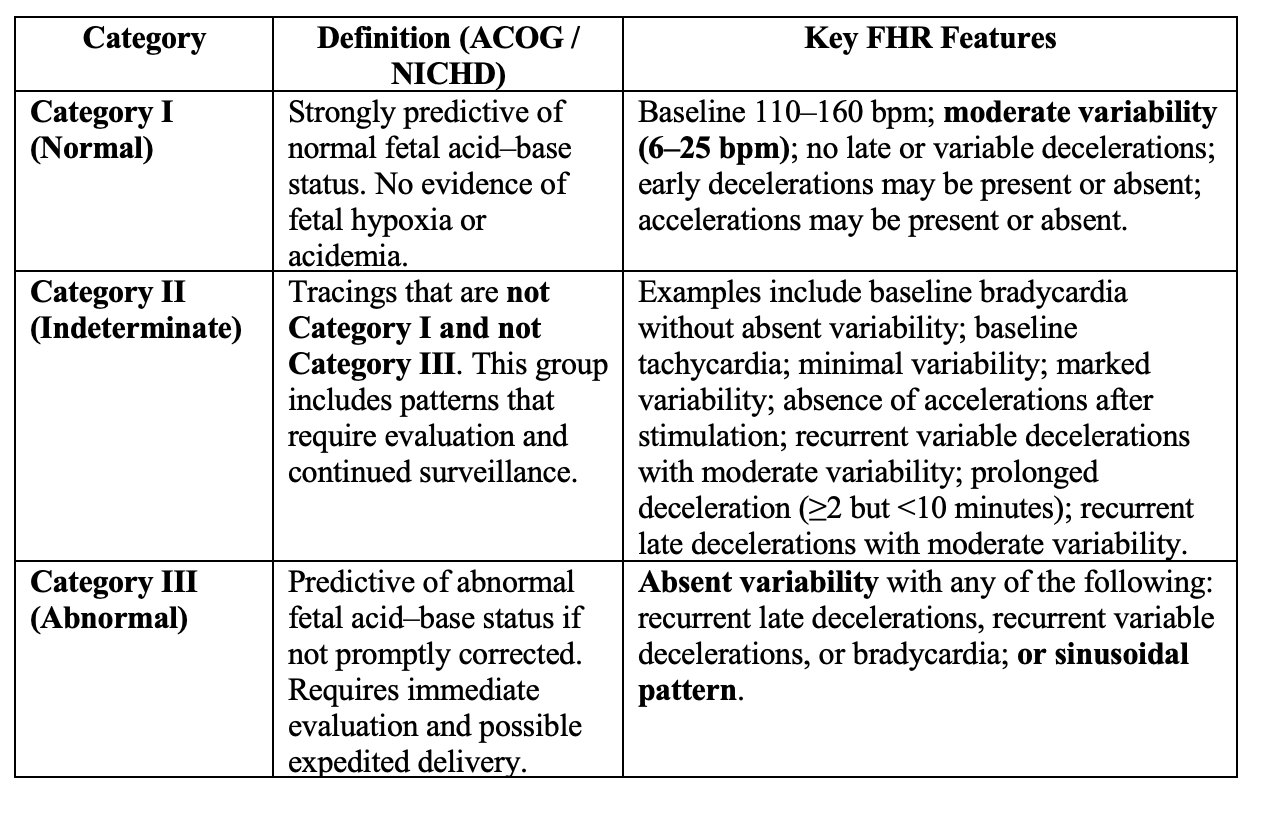
ACOG Practice Bulletin No. 106. Intrapartum Fetal Heart Rate Monitoring: Nomenclature, Interpretation, and General Management Principles. Obstet Gynecol. 2009;114:192–202. PMID: 19546798.
The framework created a shared language for clinicians across institutions.
From a communication perspective, this was a major step forward.
But the system was designed to describe patterns, not to predict the physiologic trajectory of labor.
The rest of this post is for paid subscribers.
The remainder of this analysis, including practical strategies to reduce malpractice risk and improve clinical decision-making, is available to subscribers who support ObGyn Intelligence.
