
On Reddit: "They Put Their Whole Hand Inside Me to Clean Me Out": What Pregnant Women Need to Know About Manual Uterine Exploration
A 29-week pregnant first-time mother posted on r/pregnant after her own mother told her that the worst part of childbirth was when the doctor “put their whole hand inside her to clean her.”

Summary
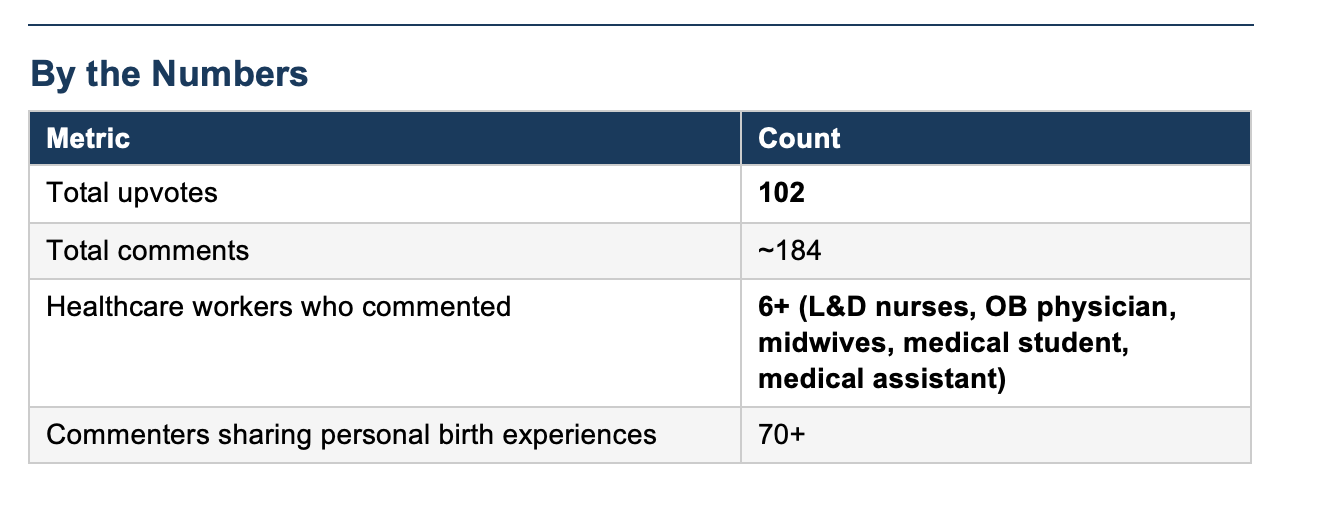
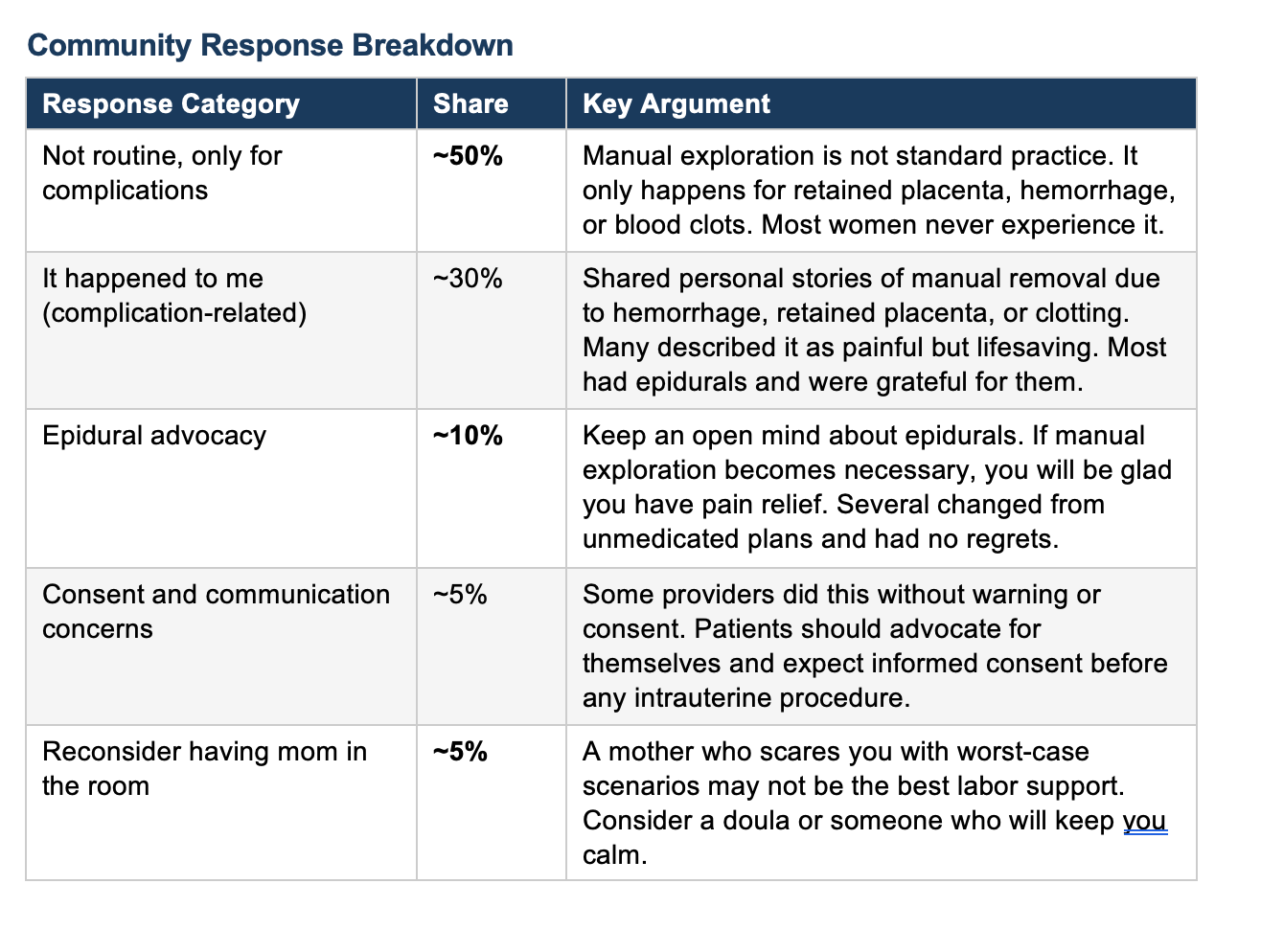
A 29-week pregnant first-time mother posted on Reddit r/pregnant after her own mother told her that the worst part of childbirth was when the doctor “put their whole hand inside her to clean her.” The poster was alarmed and turned to the community for reassurance. She is planning an unmedicated birth and wanted to know if this is something that routinely happens. The thread quickly filled with responses from L&D nurses, an OB physician, midwives, and dozens of mothers sharing their own experiences. The consensus was clear: manual uterine exploration is not routine. It is performed only when there is a complication such as a retained placenta, heavy bleeding, or clotting. The top-voted comment, from an L&D nurse with 479 upvotes, confirmed that providers typically wait up to 30 minutes for the placenta to deliver on its own, and most placentas come out well before that.
The Procedure: Manual Uterine Exploration
Manual uterine exploration is a procedure in which a provider inserts a gloved hand through the vagina and cervix into the uterus after delivery. It is not a routine part of childbirth. The most common reasons it is performed are retained placenta (when all or part of the placenta does not come out on its own within about 30 minutes), postpartum hemorrhage (heavy bleeding that does not respond to uterine massage or medications like oxytocin), and removal of large blood clots that are preventing the uterus from contracting. In some cases, providers also perform a “uterine sweep” to check that no tissue has been left behind, though this is not standard at most institutions.
The procedure can be very painful, especially if epidural anesthesia is not in place. When it is anticipated, providers can offer IV pain medication (such as fentanyl), nitrous oxide, or regional anesthesia. In some cases, the patient is taken to the operating room for the removal under spinal or general anesthesia. Retained placenta occurs in roughly 1 to 3 percent of vaginal deliveries. When it does happen, manual removal is sometimes the only option short of surgery. It is a potentially lifesaving intervention, particularly when hemorrhage is involved.
The critical point for patients: this procedure requires informed consent. Your provider should explain what they are about to do, why it is necessary, and what your options are for pain relief before proceeding. It should never come as a surprise.
What It Means
This thread captures a common problem in prenatal preparation: birth stories from family members, often told with the best of intentions, can create disproportionate fear about rare complications. The poster’s mother likely experienced a retained placenta or postpartum hemorrhage and had manual removal performed. That is a real and sometimes frightening experience. But it happens in only 1 to 3 percent of births, and presenting it as a routine part of delivery does a disservice to expectant mothers. What was encouraging in this thread was how quickly healthcare professionals stepped in with accurate information. The OB physician who commented confirmed manual exploration is reserved for hemorrhage and retained tissue, and that IV pain medication is offered if no epidural is in place. Multiple commenters who had experienced it described it as painful but brief, and those with epidurals reported feeling little to nothing.
My Take
Two things stand out from a clinical perspective.
First, the consent issue.
Several commenters described manual uterine exploration being performed without warning, without explanation, and without pain relief. One described a provider who attempted a manual rotation of an occiput posterior baby without informed consent. Another described stitching that began before local anesthesia had taken effect. These are not acceptable practices.
Informed consent is not optional, even in urgent situations.
Second, this thread illustrates why prenatal education needs to include honest discussion of the third stage of labor. That is preventive ethics.
Most childbirth preparation focuses on contractions and pushing. Very little time is spent on placental delivery, the possibility of retained tissue, or what happens if the uterus does not contract properly afterward. When patients understand the third stage, they are better prepared to participate in decisions if complications arise, rather than being blindsided by procedures they have never heard of.
Again an excellent topic. For many years when manual removal or exploration was done many physicians did not make sure patient was informed and pain meds provided. This is critical unless there is a true emergency. But as I have said before, informing patients about all these possibilities and choices ahead of time is impractical, not really helpful and potentially harmful.
Most women do not want to hear all the complications and even when they are informed about certain ones earlier in pregnancy it is usually not recalled or doesn’t prepare them in a meaningful way
We spend more time than ever counseling about so many aspects and options in pregnancy that adding more is not realistic