
Neurodevelopmental Outcomes After Forceps, Vacuum, and Second-Stage Cesarean Delivery
JAMA Netw Open.

Rajasingham M, Lisonkova S, Razaz N, Muraca GM. Long-Term Neurodevelopmental Outcomes After Forceps, Vacuum, and Second-Stage Cesarean Delivery. JAMA Netw Open. 2026;9(1):e2556637.
The Key Numbers
504,380 full-term, singleton children born in British Columbia between 2000 and 2019, followed for up to 22 years. Median follow-up: 11.6 years for ADHD, 12.5 years for ASD, 12.6 years for intellectual disability.
How they were born:
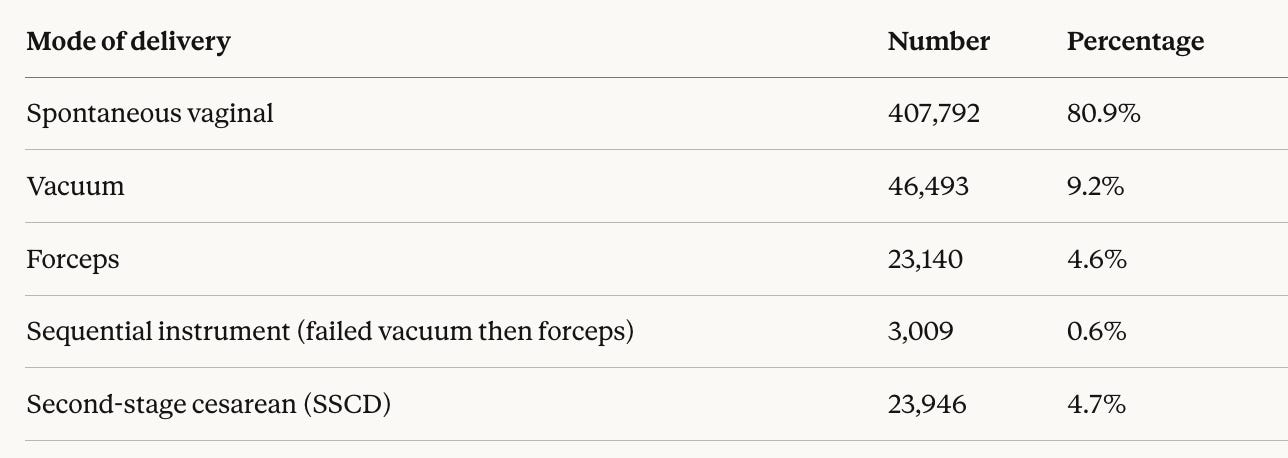
Overall rates per 1,000 person-years: ADHD 6.6, ASD 1.8, intellectual disability 0.3.
Using SSCD as the reference group (the appropriate comparator, since these are all second-stage interventions):
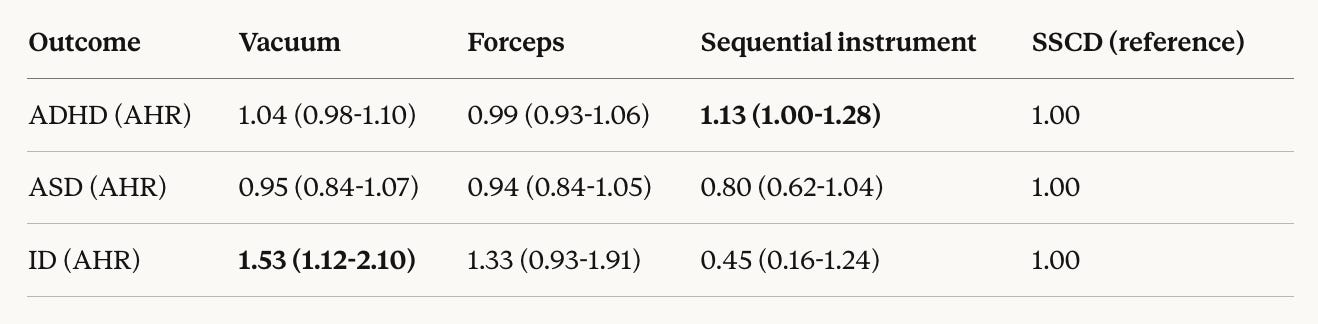
Bold = statistically significant.
What Works (The Evidence)
This study does something most previous research failed to do: it compares the right groups. Most prior studies lumped all cesareans together vs. all vaginal deliveries, a comparison so contaminated by confounding by indication that the results are nearly meaningless. A prelabor elective cesarean for breech is nothing like an emergency second-stage cesarean for arrest of descent. Comparing them as if they’re the same thing is like comparing aspirin to chemotherapy because both are “medications.”
By restricting to second-stage deliveries only, this study compares women who were all in the same clinical situation: fully dilated, needing an intervention. That’s the real decision point in labor. When a baby is stuck at full dilation, the choice is forceps, vacuum, or cesarean. This study tells us what happens to the children long-term depending on which path is taken.
The main finding: outcomes are largely comparable. Forceps delivery showed no significant difference from SSCD for ADHD, ASD, or intellectual disability. That matters, because forceps have been under siege for decades, with declining training and rising fear of litigation.
Sequential instrument delivery (failed vacuum converted to forceps) was associated with a 13% higher ADHD rate. But this involved only 0.6% of all births, and the lower confidence interval boundary was 1.00, right at the line of significance. This finding was sensitive to model specification: when smoking status was removed, the association was no longer significant (AHR 1.12, 95% CI 0.99-1.27).
Vacuum delivery showed a 53% higher rate of intellectual disability compared to SSCD. That sounds alarming until you look at the absolute numbers: the rate was 0.3 per 1,000 person-years for vacuum vs. 0.2 per 1,000 person-years for SSCD. The absolute difference is 0.1 per 1,000 person-years. And when analyzed using an intention-to-treat framework (comparing attempted vacuum vs. attempted forceps regardless of success), this association disappeared.
No delivery mode was associated with a higher rate of ASD. This is consistent with prior literature showing that the cesarean-ASD association found in earlier studies was likely explained by familial confounding, not the delivery itself.
Evidence Gaps
The ASD diagnostic algorithm in BC administrative databases has known low sensitivity, meaning ASD cases were underrepresented. This wouldn’t create a false difference between groups, but it limits the ability to detect small real differences.
BMI was missing for 26% of the cohort, though sensitivity analyses with multiple imputation didn’t change results. Sociodemographic data (race, ethnicity, income, education) were unavailable, a significant limitation given the known association between socioeconomic factors and neurodevelopmental diagnoses. Practitioner preference patterns, which influence who gets forceps vs. vacuum vs. cesarean, couldn’t be accounted for. The study didn’t examine children with multiple neurodevelopmental diagnoses, which is common in this population.
Perhaps most importantly: the women who got SSCD had higher rates of obesity, gestational diabetes, gestational hypertension, and longer labors. Despite adjusting for these, residual confounding could mean SSCD outcomes are slightly worse than they appear, which would further narrow the gap between operative vaginal delivery and SSCD.
Bottom Line
When researchers ask the right question, they get a different answer than the one that has dominated obstetric discourse for years. The right question is not “are cesareans safer than vaginal birth?” It is: “when a baby needs help getting out during the second stage, which intervention produces the best long-term outcomes for the child?”
This study’s answer: it largely doesn’t matter. Forceps, vacuum, and second-stage cesarean produce comparable neurodevelopmental outcomes over 22 years of follow-up.
The small signals (sequential instruments and ADHD, vacuum and intellectual disability) are either clinically marginal in absolute terms or sensitive to analytical approach.
For clinicians, this is reassuring. The choice between operative vaginal delivery and SSCD should be guided by the clinical situation, maternal preference, and operator skill, not by fear that one mode will harm the child’s brain development. For the ongoing debate about whether the decline in forceps training is harming patients, this study provides indirect support for maintaining operative vaginal delivery skills: forceps showed the cleanest safety profile of all operative modes.
For patients, the message is straightforward: if your baby needs help being born during the pushing stage, the available options are comparably safe for your child’s long-term development. Ask your doctor which option they are most skilled at and which best fits your clinical situation.
Reference:
Rajasingham M, Lisonkova S, Razaz N, Muraca GM. Long-Term Neurodevelopmental Outcomes After Forceps, Vacuum, and Second-Stage Cesarean Delivery. JAMA Netw Open. 2026;9(1):e2556637. doi:10.1001/jamanetworkopen.2025.56637