

In aviation accident investigation, conclusions are never based on a brief case description or on the most visible failure at the end of an event. Investigators from the National Transportation Safety Board reconstruct the entire chain of events.
They establish a precise timeline, examine the technical and human factors involved, and identify the initiating event that began the sequence leading to the crash.
Only after this disciplined reconstruction do they determine the probable cause and propose safety recommendations.
Adverse events in obstetrics deserve the same analytical rigor. Too often, clinical discussions begin with a presumed cause and then work backward to justify it. A structured approach forces investigators to do the opposite: reconstruct the facts first and determine causation only after the full physiologic and clinical sequence is understood. The following framework adapts principles from aviation accident investigation to obstetric cases and can help clinicians analyze complex events more objectively.
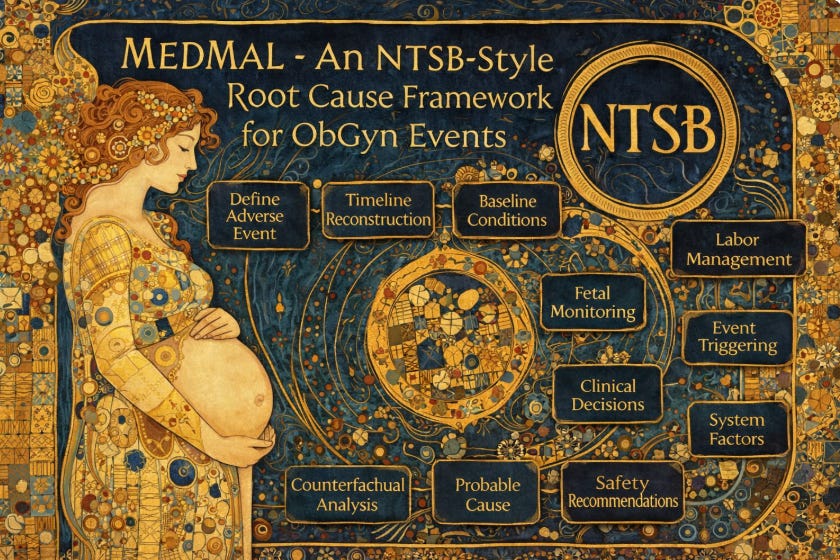
An NTSB-Style Root Cause Framework for Obstetric Events
1. Define the event clearly
What exactly happened? For example, neonatal HIE, maternal hemorrhage, uterine rupture, or unexpected fetal death.
2. Reconstruct the complete timeline
Build a precise minute-by-minute chronology antenatally not only from admission through the adverse outcome.
3. Baseline maternal and fetal condition
Maternal comorbidities, gestational age, fetal growth, antenatal testing, and initial fetal heart rate status.
4. Indication for labor or intervention
Why was the patient in labor or undergoing induction or augmentation?
5. Labor management details
Induction agents, oxytocin dosing, membrane rupture, cervical progress, uterine activity, and staffing.
6. Fetal monitoring evolution
Baseline tracing characteristics, variability, decelerations, and classification before the critical event.
7. Triggering event
Identify the physiologic event that initiated deterioration. Examples include tachysystole, cord compression, placental abruption, uterine rupture, or maternal hypotension.
8. Physiologic progression
How did the fetal or maternal condition evolve after the trigger? What objective data document this progression?
9. Clinical decision points
What decisions were made, when were they made, and what information was available to clinicians at that moment?
10. System and resource factors
Staffing levels, anesthesia availability, operating room readiness, communication pathways, and institutional protocols.
11. Counterfactual analysis
At what point could a different action plausibly have changed the outcome?
12. Probable cause and prevention
Identify the initiating cause and contributing factors. Then determine what system changes could realistically reduce recurrence.
The key lesson mirrors aviation accident investigation: the visible failure at the end of a sequence is often not the root cause. Only after reconstructing the entire chain of physiologic and clinical events can the true cause be identified.
The rest of this post is for paid subscribers.
Continue reading for the full checklist.
Access is reserved for subscribers who want the complete evaluation.
Complete 200 Point Checklist for Root cause analysis of an adverse ObGyn Event. PLUS 15 Preventative Questions.
