
Induction Tips Thread
The Induction Preparation Guide Your OB Didn't Provide

Original Post Summary
This is an r/pregnant Reddit post. A first-time mother at 40 weeks + 4 days with an uneventful pregnancy seeks advice before her scheduled induction. Despite a healthy pregnancy, she remains only 1cm dilated with no option for membrane sweeping. Her OB scheduled a Sunday night induction starting with cytotec (misoprostol), anticipating approximately 24 hours of labor. While expressing disappointment about not experiencing spontaneous labor, she maintains a positive outlook and asks the community for practical tips and things they wish they had known before their own inductions.
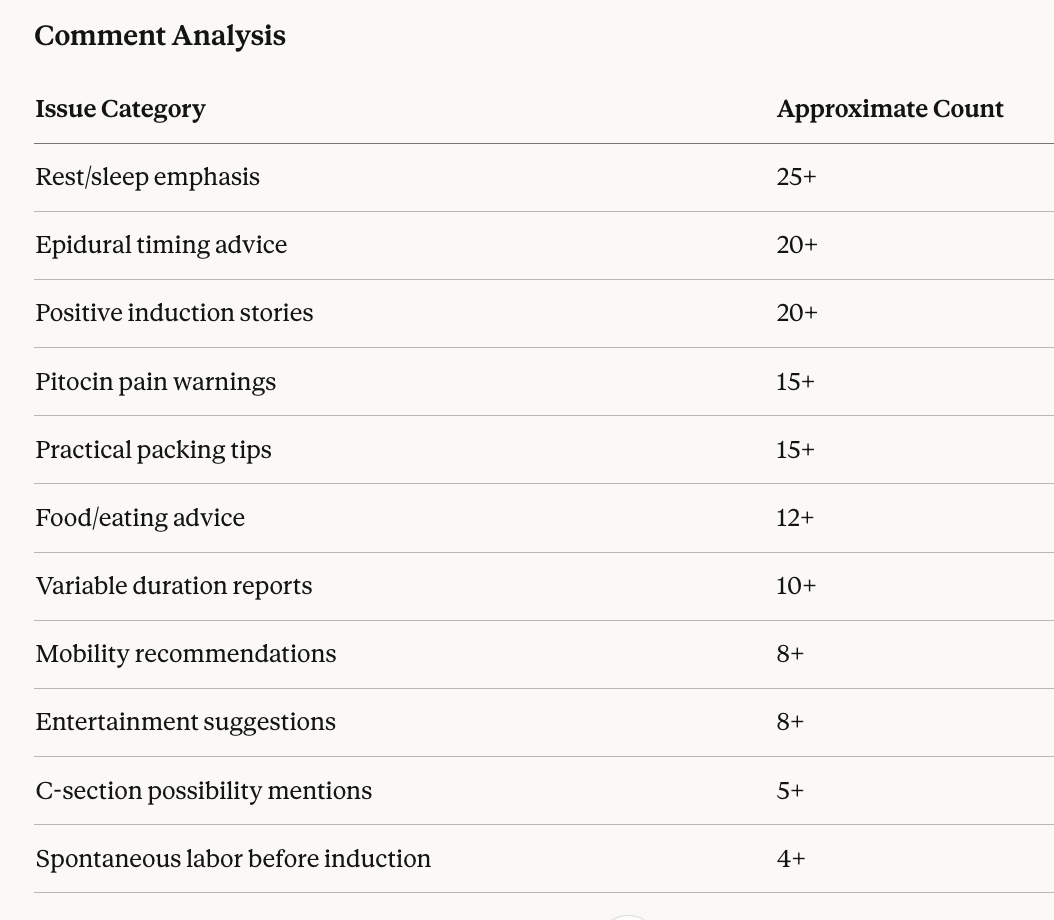
Comment Summary (78 comments)
The thread generated an overwhelmingly supportive response with practical advice spanning preparation, pain management, epidural timing, and emotional readiness. Comments ranged from brief encouragement to detailed birth narratives, with a notable emphasis on countering negative induction narratives with positive experiences.
Preparation Advice (25+ comments) The most consistent recommendation across comments was prioritizing rest before admission. Multiple commenters emphasized that induction can span 24-48+ hours, making pre-admission sleep critical. One commenter noted going from Friday evening to Sunday morning without real sleep. Practical packing suggestions included entertainment (books, streaming devices, word puzzles), personal comfort items (own pillows, robes, slippers, toiletries), and snacks for both during and after labor. Several noted hospital food inadequacy and recommended protein bars and jerky for sustained energy.
Food timing received significant attention. Multiple commenters advised eating a substantial meal before admission since many hospitals restrict patients to clear liquids once active labor begins, particularly after epidural placement. One commenter specifically noted being placed on a broth-only diet after her epidural.
Epidural Timing Debate (20+ comments) The thread revealed substantial disagreement about optimal epidural timing, reflecting genuine medical uncertainty. Several commenters shared experiences of resisting epidurals for 20+ hours based on fears of labor stalling, only to find the epidural actually accelerated dilation. One reported progressing from 5cm to 10cm after epidural placement. Another went from 3cm to 9cm in 2 hours post-epidural. A midwife in the thread explained that epidural-induced relaxation can help tense patients progress faster.
Conversely, one commenter explicitly stated she got her epidural too early and it prolonged everything by 18 hours, advising others to wait until further dilated if possible.
The more consistent advice: if you plan to get an epidural, request it before intense contractions make positioning difficult. Multiple commenters described struggling to hold still during epidural placement due to severe pain. One specifically warned that with pitocin inductions, contractions arrive suddenly and intensely, making the anesthesiologist wait time (sometimes 90+ minutes) excruciating.
Pitocin Pain Reality (15+ comments) A recurring theme was that pitocin-induced contractions differ qualitatively from spontaneous labor contractions. One midwife explained the physiological reason: natural oxytocin crosses the blood-brain barrier, triggering endorphin release for natural pain relief. Synthetic pitocin does not cross this barrier, resulting in more intense pain without compensatory endorphin response.
Multiple commenters described pitocin contractions as arriving like a “freight train” without the gradual buildup of natural labor. One commenter made it to 6cm before epidural but wished she’d gotten it sooner. Another described the worst pain of her life during the 90-minute wait for anesthesiology after requesting epidural.
Positive Induction Narratives (20+ comments) A notable feature of this thread was explicit pushback against negative induction narratives. One L&D nurse who had two elective 39-week inductions stated both were “perfect” and she’d choose induction again for a third pregnancy. Another commenter reported going from 2cm to 10cm in under 2 hours and pushing for 15 minutes. Multiple commenters described total labor times under 6 hours.
Several specifically noted that induction allowed them to plan, prepare the home, pack appropriately, and arrive rested. One pointed out the psychological benefit of knowing exactly when labor would begin rather than experiencing unpredictable onset.
A friend’s story was shared of progressing from 1cm to 9cm in one hour as a first-time mother, with nurses shocked when a practice push revealed the baby’s head immediately visible.
Variable Duration Reports Labor durations reported in comments ranged dramatically: 2 hours, 4 hours, 6 hours, 10 hours, 15 hours, 17 hours, 26 hours, 44 hours, and 4 days (using sequential methods). Starting dilation appeared to influence duration, with several noting that arriving at 4cm resulted in much faster progression. One commenter at 1cm dilated had a 6-hour intense labor, while another at 1cm reported 44 hours.
Induction Methods Discussed Comments referenced multiple ripening and induction agents: cytotec/misoprostol (oral or buccal), cervical pessaries, Foley balloon catheters, cervidil, and pitocin. Several women required multiple rounds of cervical ripening before active labor. One commenter had 3 rounds of cytotec (12 hours total) before pitocin even started. Another was induced for 4 days across three methods. The Foley balloon generated some discussion, with an L&D nurse clarifying that most women tolerate it without epidural, contrary to one commenter’s suggestion to request epidural before balloon placement.
Mobility and Positioning (8+ comments) Several commenters emphasized staying mobile and upright as long as possible. Recommendations included using birth balls, walking, and rotating positions. The peanut ball received specific mention as helpful for women confined to bed with epidurals. One commenter suggested asking about wireless monitoring to allow movement while maintaining fetal surveillance.
Unexpected Outcomes (5+ comments) A few commenters shared that their bodies went into spontaneous labor before scheduled inductions, sometimes on the induction date itself. One woman noted both her scheduled inductions resulted in spontaneous labor starting on the appointment day. Another went from scheduled induction to active labor over the weekend before her appointment.
Several mentioned that induction doesn’t guarantee vaginal delivery. One labored 17 hours before cesarean due to baby’s position and inability to establish contraction patterns. The thread maintained a realistic but non-alarmist tone about this possibility.
Analysis
This thread represents peer support functioning as intended, with experienced mothers sharing practical wisdom that healthcare systems often fail to provide. The collective knowledge addresses gaps in standard prenatal education, where induction procedures may be explained medically but lived experience remains inaccessible.
Several professional accountability observations emerge:
Informed Consent Adequacy: The sheer volume of “I wish I’d known” comments suggests systematic gaps in pre-induction counseling. When dozens of women report surprise at pitocin pain intensity, epidural timing constraints, or multi-day induction possibilities, the informed consent process warrants examination. Patients scheduled for induction should receive explicit discussion of: realistic duration ranges (2-48+ hours), qualitative differences between induced and spontaneous contractions, epidural timing considerations and anesthesiology availability, food and activity restrictions, and cesarean possibility statistics for inductions at various starting conditions.
Pain Management Communication: The epidural timing debate reveals a communication failure. Patients arrive with conflicting information (epidurals stall labor vs. epidurals enable progress) and receive insufficient guidance for their specific clinical situation. The commenter who waited 90 minutes in severe pain for anesthesiology represents a systems failure, not personal miscalculation.
Expectation Setting: The original poster’s OB anticipated 24-hour labor. Thread responses suggest this estimate, while reasonable, may not prepare patients for the genuine possibility of 40+ hour inductions. Under-promising duration creates unnecessary anxiety when labor extends; realistic range communication respects patient autonomy.
Positive Observation: Unlike threads documenting traumatic care, this discussion reflects women feeling empowered to advocate for themselves within the medical system. Commenters describing epidural requests, snack smuggling, and entertainment preparation demonstrate patients actively managing their experience rather than passively receiving care.